
I have been advocating in the Northern Territory for changes in the way doctors present themselves to patients. I want to see transparency of a doctor’s registration status so that patients are aware of who is working under supervision and the name of that doctor’s supervisor. That way patients can escalate any issues to a supervisor if they are not satisfied with the care they are being offered.
Currently in Australia patients have to go to the AHPRA website and look up their doctor. Also, the doctor’s supervisor is not named on that site. How are patients to know who they are dealing with?
I propose the use of 3 colours – red, orange and green – to represent registration status based on supervision requirements. These would have the following meaning:
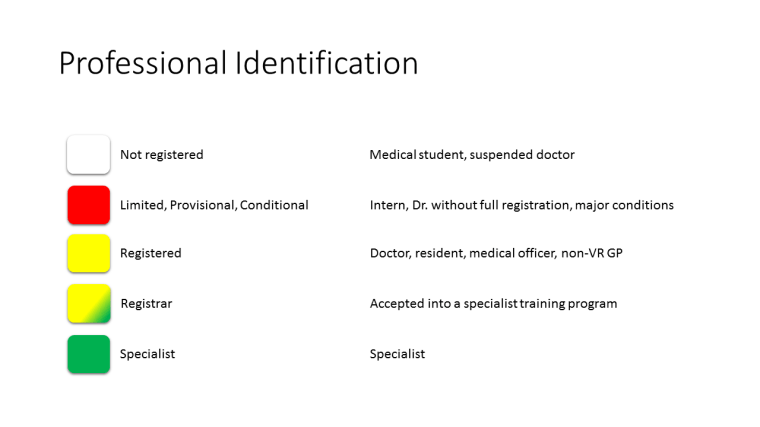
Doctors accepted into a formal training program would be recognised by a mixture of yellow and green.
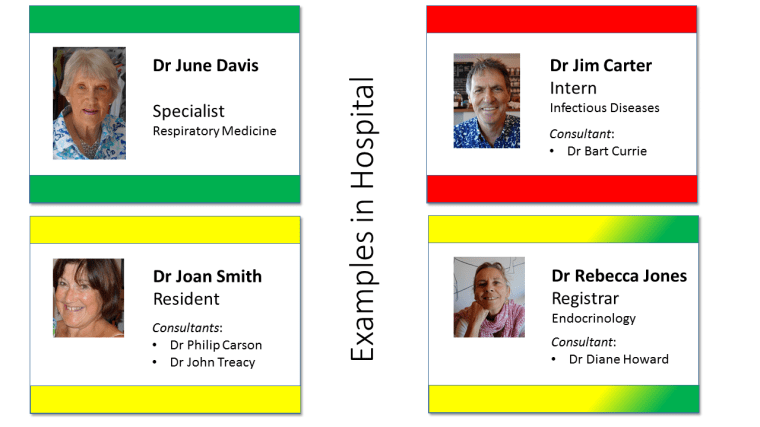
Badges might look like this in hospitals:
And like this in primary care:
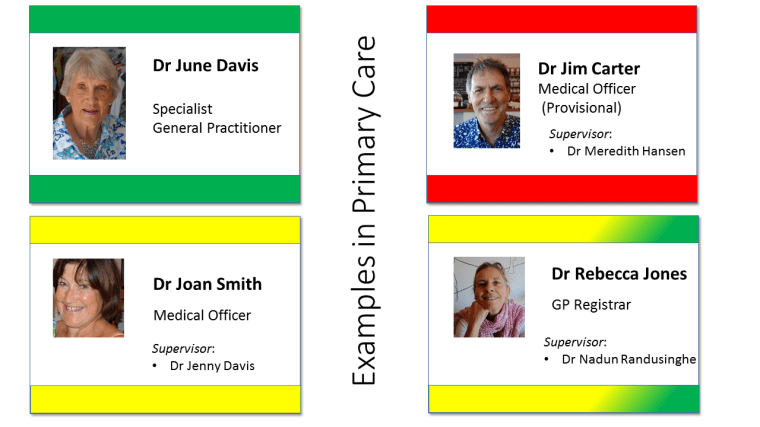
In general practice the colours could be on the name tag on the door rather than on a badge. The point is that patients could understand where we all fit into the world of medicine, whether in hospital or primary care.
Let’s make it clear for patients. The current universal response by doctors to this challenge is that patients have “no idea about the registration status of doctors”. Well, who is to blame for that? I am certain that they want to know.

Interesting concept, thanks Sam.
I like the underlying sentiment of providing patients with more information, although I think your colour coding is a bit of a distraction. I suspect, if you did a survey after the introduction of the colour code (even years after), most patients would have no idea what a purple-and-green code meant, for example. I work for Qld Health, which has about six emergency colour codes and I couldn’t say for certain what any of them means, without looking at a ‘cheat sheet’.
I think your concept of openly naming the registration status is important, though.
‘Med student’ needs no change.
‘GP Registrar’ needs no change
What remains, then, is the need to distinguish a Specialist GP from a doctor working in primary care who has no primary care qualification. This would only work if it became a regulated rule, and I think it is highly unlikely any ruling body would be able to ban the untrained from calling themselves a GP – it is so ingrained.
Therefore, the main issue, I think, is to create a new term such as Specialist GP which no one else is allowed to use. It is easier to control a new term than to try to change the rules around an age-old one such as GP.
The terms ‘specialist’ and ‘general’ do unfortunately create somewhat of an oxymoron, in that they mean almost the opposite of each other. So I’m not sure what the term should be, but ultimately it should distinguish a GP who has completed their postgrad primary care training.
Once you have that term fixed, it becomes easier to educate patients.